Overview
The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed.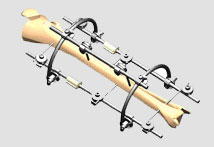
Causes
Leg length discrepancies can be caused by: hip and knee replacements, lower limb injuries, bone diseases, neuromuscular issues and congenital problems. Although discrepancies of 2 cm or less are most common, discrepancies can be greater than 6 cm. People who have LLD tend to make up for the difference by over bending their longer leg or standing on the toes of their shorter leg. This compensation leads to an inefficient, up and down gait, which is quite tiring and over time can result in posture problems as well as pain in the back, hips, knees and ankles.
Symptoms
As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies.
Diagnosis
A qualified musculoskeletal expert will first take a medical history and conduct a physical exam. Other tests may include X-rays, MRI, or CT scan to diagnose the root cause.
Non Surgical Treatment
In an adult, we find that we can add a non compressive silicone heel lift to a shoe in increments of 3-4 mm maximum per week. Were we to give a patient with a 20 mm short leg, 20 mm of lift all at once, their entire body would rebel. The various compensations that the body has made, such as curvatures and shortening of muscles on the convex side of the curve, would make such a dramatic change not just noticeable, but painful. When we get close to balancing a patient by lifting a leg with heel inserts, then we perform another gait analysis and follow up xray. At that point, we can typically write them a final prescription to have their shoe modified. A heel lift is typically fine up to 7 mm. When it gets higher than that, the entire shoe must be modified. There are two reasons for this. The back of the shoe is generally too short to accommodate more than 7-8 mm inserted inside the shoes and a heel lift greater than 7 mm will lead to Achilles tendon shortening, which then creates it?s own panoply of problems.

how to increase height naturally after 18
Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
The bone is lengthened by surgically applying an external fixation device to the leg. The external fixator, a scaffold-like frame, is connected to the bone with wires, pins, or both. A small crack is made in the bone and the frame creates tension when the patient or family member turns its dial. This is done several times each day. The lengthening process begins approximately five to 10 days after surgery. The bone may lengthen 1 millimeter per day, or approximately 1 inch per month. Lengthening may be slower in a bone that was previously injured. It may also be slower if the leg was operated on before. Bones in patients with potential blood vessel abnormalities, such as cigarette smokers, may also need to be lengthened more slowly. The external fixator is worn until the bone is strong enough to support the patient safely. This usually takes about three months for each inch. Factors such as age, health, smoking and participation in rehabilitation can affect the amount of time needed.
Causes
Leg length discrepancies can be caused by: hip and knee replacements, lower limb injuries, bone diseases, neuromuscular issues and congenital problems. Although discrepancies of 2 cm or less are most common, discrepancies can be greater than 6 cm. People who have LLD tend to make up for the difference by over bending their longer leg or standing on the toes of their shorter leg. This compensation leads to an inefficient, up and down gait, which is quite tiring and over time can result in posture problems as well as pain in the back, hips, knees and ankles.
Symptoms
As patients develop LLD, they will naturally and even unknowingly attempt to compensate for the difference between their two legs by either bending the longer leg excessively or standing on the toes of the short leg. When walking, they are forced to step down on one side and thrust upwards on the other side, which leads to a gait pattern with an abnormal up and down motion. For many patients, especially adolescents, the appearance of their gait may be more personally troublesome than any symptoms that arise or any true functional deficiency. Over time, standing on one's toes can create a contracture at the ankle, in which the calf muscle becomes abnormally contracted, a condition that can help an LLD patient with walking, but may later require surgical repair. If substantial enough, LLD left untreated can contribute to other serious orthopaedic problems, such as degenerative arthritis, scoliosis, or lower back pain. However, with proper treatment, children with leg length discrepancy generally do quite well, without lingering functional or cosmetic deficiencies.
Diagnosis
A qualified musculoskeletal expert will first take a medical history and conduct a physical exam. Other tests may include X-rays, MRI, or CT scan to diagnose the root cause.
Non Surgical Treatment
In an adult, we find that we can add a non compressive silicone heel lift to a shoe in increments of 3-4 mm maximum per week. Were we to give a patient with a 20 mm short leg, 20 mm of lift all at once, their entire body would rebel. The various compensations that the body has made, such as curvatures and shortening of muscles on the convex side of the curve, would make such a dramatic change not just noticeable, but painful. When we get close to balancing a patient by lifting a leg with heel inserts, then we perform another gait analysis and follow up xray. At that point, we can typically write them a final prescription to have their shoe modified. A heel lift is typically fine up to 7 mm. When it gets higher than that, the entire shoe must be modified. There are two reasons for this. The back of the shoe is generally too short to accommodate more than 7-8 mm inserted inside the shoes and a heel lift greater than 7 mm will lead to Achilles tendon shortening, which then creates it?s own panoply of problems.
how to increase height naturally after 18
Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
